Why an induction of labour may be offered or advised
Options for starting labour and induction of labour
Options for starting labour
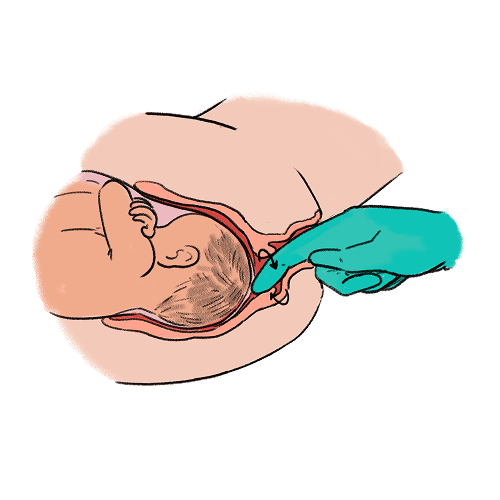
Before your induction: Membrane sweep
Before inducing labour, you’ll be offered a membrane sweep (1), to increase chances of going into spontaneous labour. To perform this, your midwife or doctor will perform a vaginal examination by inserting their finger through the neck of your womb (cervix) and using circular movements, separate the membranes of the amniotic sac surrounding your baby from the neck of your womb (cervix), which releases hormones (prostaglandins), which help to start your labour.
Some women find the procedure uncomfortable or painful. You may get some cramping and mild vaginal bleeding afterwards. A membrane sweep can be usually offered to you after 39+0 weeks. If labour does not start after your first membrane sweep, you may be offered an additional sweep.
Methods of induction of labour:
Induction of labour is designed to induce the onset of labour by softening and maturing the neck of your womb (cervix) and stimulate contractions. There are a variety of methods available for inducing labour, both medical treatments and mechanical methods.
The choice of the method depends on:
The readiness of your cervix (assessed using a vaginal examination and calculating a Bishop score)
Whether your waters have broken
Your preferences.
What is Bishop score?
The Bishop score is a number obtained by doing a vaginal examination, and is based on:
How many cm dilated you are – dilatation is from closed – 10cm.
Length (effacement) of the neck of your womb (cervix) – effacement is long (0%) – paper thin (>80%)
Position of the neck of your womb (cervix) in your vagina – position goes from posterior to anterior during labour.
Consistency of the neck of your womb (cervix) – consistency goes from firm to soft during labour.
How far down the pelvis your baby’s head is (station) – station starts at -3 (high) to +2 (at the vaginal entrance).
When your Bishop score is 6 or less you will be offered:
Medication to ripen the neck of your womb (cervix).
Mechanical method (a balloon inserted into the neck of your womb).
When your Bishop score is more than 6, you will be offered:
Breaking your waters (amniotomy) and giving a hormone (oxytocin) drip through a vein in your arm.
Different methods for inducing labour
Medication for induction:
There are various medications available to induce your labour.
The medication used for induction is called prostaglandin.
There are several different types of prostaglandins that can induce labour. They are usually given vaginally but may sometimes be given to you by mouth (orally). Prostaglandins usually take 12-24 hours to ripen the neck of your womb (cervix). This depends on the type of prostaglandin, its dose and how ready the neck of your womb (cervix) is. Talk to your team about which prostaglandin they use in your hospital.
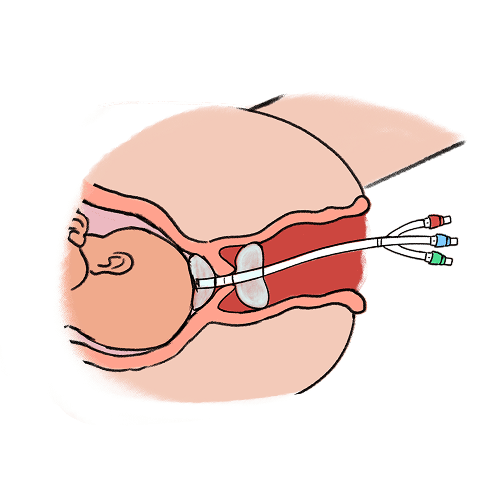
Mechanical methods of Induction of labour:
Mechanical methods for induction stretch the neck of your womb (cervix) promoting hormone release. This can be done by using either a balloon catheter or osmotic dilators.
A balloon catheter is inserted into the canal in your cervix to reach the space inside the womb just outside the amniotic sac covering your baby and inflated with water to hold it in place, after which the cervix gradually dilates and releases hormones which can induce the onset of labour.
An osmotic dilator is a medical device used to dilate the cervix by swelling as it absorbs fluid from the surrounding tissue in your body
Mechanical methods of induction of labour usually work within 24 hours. Talk to your team about how long it will stay in for.
Mechanical methods of induction of labour are safe for you and your baby and they are as effective as vaginal medication at inducing labour.
Induction with a mechanical device in the neck of your womb is less likely to cause excessive contractions than vaginal medication. It is recommended to opt for this method of induction if you have had a previous caesarean birth. Talk to your team about the option that is best for you and your circumstances.
Prostaglandin Pessary

Prostaglandin Gel
Balloon Dilator
Breaking of the waters (amniotomy) and the hormone drip (oxytocin):
When your cervix is examined and it is deemed appropriate to break your waters (artificial rupture of membranes/amniotomy), this will be undertaken on the delivery suite. You will be offered a hormone drip (oxytocin). You can choose to have this immediately or delay starting to see if you contract regularly after breaking your waters. Any delay may lengthen your labour and may increase the chance of your baby developing an infection.
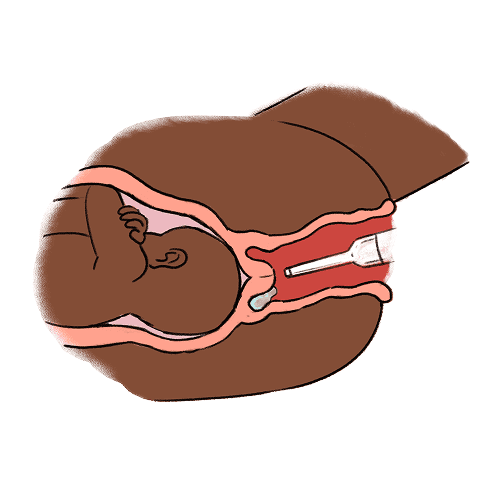
Breaking your waters (amniotomy):
Breaking of the waters (artificial rupture of the amniotic membranes or amniotomy) is part of the induction process if your waters haven’t broken spontaneously. It is also performed during spontaneous labour if progress slows down. It may increase the strength and number of contractions you have therefore shortening labour by about an hour. It does not involve giving any medication, the process involves the puncturing of the membranes with a crochet‐like long‐handled hook during a vaginal examination.

Breaking your waters (amniotomy/artificial rupture of membranes)
After breaking your waters, your contractions may speed-up and you may experience more pain. Once your waters are broken, if your progress in labour is slower this may increase the chances of your baby developing an infection.
Hormone drip (Oxytocin)
A hormone medication called oxytocin can be used to increase the amount and strength of your contractions. We would need to monitor your baby’s heart rate and your contractions continuously while its given using CTG (cardiotocography). Using the hormone drip may shorten the length of your labour. It does not affect your mode of birth or your baby’s condition.
Oxytocin may cause you to contract too frequently (uterine hyperstimulation), this is more painful for you and may reduce oxygen to your baby temporarily, if this happens for too long your baby may show signs of distress on the heart rate monitor (CTG). The senior members of the team will need to review you and may reduce or stop the hormone drip (oxytocin), if your contractions continue despite this, we can give you medication (tocolytic) to resolve this. These measures will give your baby more time to recover between contractions by slowing them down and making them more regular and effective.
If labour does not start despite being induced, a doctor will discuss with you what your options are going forward. They will review your pregnancy notes and the baby’s latest heart rate (CTG) trace. Depending on your specific case they may offer you:
Further attempt at inducing labour – this may include trying to induce you using a different method than was originally used.
A period of rest after which we will re-examine the neck of your womb (cervix) to see if there has been any change.
Awaiting events i.e. seeing if you go into active labour on your own.
A Caesarean birth.
Almost 1 in 3 women in the UK will have their labour induced. Although over half result in active labour and a vaginal delivery, for some women this is not the case.
We do not always know why active labour may not happen for you following induction, however we put you and your baby at the centre of our care and you making an informed decision about your care is most important to your team.
Alternative therapies and methods of starting labour
There are multiple alternative/other therapies described in literature as alternative methods for induction of labour. Currently, available guidance from NICE does not support the use of non-pharmacological methods for induction of labour including herbal supplements, acupuncture, homeopathy, castor oil, hot baths, enemas, sexual intercourse. The main reasons for this are due to the lack of available evidence in evaluating the effectiveness of these methods.
Recommendations | Inducing labour | Guidance | NICE
Raspberry leaf tea
Raspberry leaf is frequently used during pregnancy and labour to strengthen and tone the uterus, theoretically assisting contractions and preventing excessive bleeding (haemorrhage). While there is a long history of raspberry leaf use in pregnancy there is little research contributing to the evidence base especially in relation to its mechanism of action, efficacy or potential harmful effects.
Raspberry leaf has demonstrated both stimulatory and relaxation effects on smooth muscle depending on a variety of factors including herbal preparation used, method of extraction, type of tissue and animal, baseline muscle tone and pregnancy status of uterus or uterine tissue. However, raspberry leaf may interact with other drugs particularly how they are broken down (metabolised) in your body.
The evidence of raspberry leaf use in pregnancy does not show any benefit. Further research is required to provide this information.
Herbal supplements:
· Herbal medications have been proposed to increase oxytocin levels and increase muscle contractility. However, most studies that have trialled the use of herbal medicines were provided at a safe environment i.e. carried out in a health facility and monitored by staff.
· The Guideline Development Group (NICE) considered that the unsupervised use of herbal preparations, which may contain active ingredients with undesirable effects, should be treated with caution. Further research is required to evaluate the effectiveness, safety and maternal satisfaction of the use of herbal supplements as a method of induction of labour.
· NICE therefore does not support the use of herbal medicines as an alternative method for the induction of labour until further safety concerns and precautions are understood.
Acupuncture/Acupressure:
Acupuncture has shown some benefit in improving cervical maturity and may increase uterine contractility and alleviate labour pain.
Acupressure uses the same points as acupuncture but applies manual pressure, usually with the finger or thumb, on these points rather than the insertion of a needle.
Many acupuncturists argue that to achieve the optimal effect of acupuncture, it is important that the treatment be customised according to the diagnostic process that is integral to the traditional Chinese system of medicine.
However, the available evidence is insufficient to determine the effectiveness of acupuncture in cervical priming/induction of labour. NICE therefore does not support the use of acupuncture as an alternative method for induction of labour.
Homeopathy:
Homeopathy involves the administration in dilution of substances aimed at the alleviation of symptoms that the same substances generally cause in their undiluted form.
It has been suggested that the herbs belonging to the Caulophyllum genus are useful in establishing labour, when uterine contractions are short and/or irregular or when they stop.
However, there is not enough evidence to show the effect of homoeopathy for inducing labour. NICE therefore does not support the use of homeopathy as an alternative method for induction of labour.
Castor oil, hot baths and enemas.
Castor oil has been widely used as a traditional method of initiating labour in midwifery practice. However, the mechanism is poorly understood. Evidence from a Cochrane systematic review and a randomised control trial suggested that women given castor oil for induction of labour achieve similar maternal and fetal outcomes as women given placebo. One small, randomised control trial reported improved “Bishop scores” in women given castor oil. However, both studies reported that castor oil was associated with nausea.
There is limited and conflicting evidence relating to the effects of castor oil for cervical priming and induction of labour. Castor oil is unpleasant to ingest and causes nausea.
There is no available evidence relating to hot baths or enemas as induction agents.
NICE does not support the use of these methods for induction of labour.
Sexual intercourse.
The role of sexual intercourse in stimulating labour is not well understood. It has been suggested that human semen is a biological source of high prostaglandin concentrations, and the action of sexual intercourse may ripen the cervix and stimulate uterine contractions. There may be an endogenous release of oxytocin as a result of orgasm. A Cochrane small study with limited data found no significant difference in labour outcomes between sexual intercourse and no sexual intercourse.
There is not enough evidence to show whether sexual intercourse is effective or to show how it compares with other methods. More research is needed.
NICE does not support sexual intercourse as a method for induction of labour.
Breast/nipple stimulation
Breast stimulation results in the production of endogenous oxytocin in both pregnant and non-pregnant women, causing uterine contractions. Evidence from a Cochrane systematic review suggested that breast stimulation appears to be beneficial in increasing the number of women in labour by 72 hours and in reducing postpartum haemorrhage rates when compared with control. Caesarean birth rates were similar between breast stimulation and intravenous oxytocin.
There is evidence that breast stimulation may be effective as a method of induction. However, interpretation of the results should be used with caution given inconsistencies with the findings and the evidence being low-quality.
Further research is required to evaluate the effectiveness, timing, methods, frequency, safety and maternal satisfaction of breast stimulation as a method of induction of labour. NICE therefore currently does not support its use as a method for induction of labour.
Hypnosis
Hypnosis is a relaxation technique in which the person closes down their awareness of external distractions to concentrate on a specific image, thoughts or feelings.
Hypnosis has long been used to reduce pain perception during labour and hypnotic relaxation may be beneficial for women who are anxious about giving birth.
A Cochrane review (2014) found no randomised control trials of acceptable quality and therefore concluded that further evidence from RCTs is required to evaluate the effectiveness and safety of this intervention for labour induction. The review also states how hypnosis may delay standard care (in case standard care is withheld during hypnosis), and its use in induction of labour should be considered on a case‐by‐case basis. No guidance has been provided specifically on hypnosis as a method for induction of labour by NICE.
Curry
Spicy foods (e.g. curry) are sometimes thought to stimulate the gut, which could hypothetically lead to uterine contractions through increased production of prostaglandins (hormones involved in labour). However, the link between dietary intake of spicy foods and significant changes in prostaglandin levels is not well-supported by research. Studies have focused on direct medical application, such as prostaglandin gels or tablets not dietary influences.
Aromatherapy
Aromatherapy involves the use of the essential oils, which are volatile, fragrant organic compounds obtained by distillation for plant material derived from roots, leaves, bark, seeds and flowers.
Aromatherapy can help in relieving maternal anxiety and pain during labour. However, there is insufficient evidence about the effectiveness of aromatherapy on pain management in labour or any primary or secondary outcome from two randomised controlled trials comparing essential oils with an active control or standard care. Additionally, there is no peer-reviewed evidence to suggest that it can be used as an alternative method for inducing labour.
Keeping active/walking
Maternal exercise has been shown to increase uterine activity. It has also been demonstrated that patients who are more physically active during pregnancy have a shorter duration of active labour.
According to the results from a randomised control trial , walking could be recommended to low-risk pregnant women to improve some of the significant outcomes of labour and delivery such as cervix preparation and Bishop Score, increasing the cases of spontaneous labour, and decreasing the cases of induction of labour and caesarean section without causing any undesirable effects on the neonate's Apgar score. The trial found that walking 40 minutes a day four times per week starting at 34 weeks improved spontaneous labour rates in 90% of women. However, the NICE and RCOG guidelines on induction of labour do not formally recommend walking as an evidence-based method to induce labour.
Vaginal douching (washing) prior to induction
The theory of vaginal douching (washing) before induction is associated with the aim of making your vagina more alkaline (increasing its pH), which may be associated with induction leading to active labour. There is conflicting evidence regarding vaginal douching (washing) before induction of labour.
The NICE guideline on induction of labour does not mention vaginal washing or douching as a method for induction.
Reflexology
Reflexologists propose that there are reflex points on the feet corresponding to organs and structures of the body and that pain may be reduced by gentle manipulation or pressing certain parts of the foot. Pressure applied to the feet has been shown to result in an anaesthetizing effect on other parts of the body. It has also been shown to potentially be effective and safe on labour pain, duration of labour, and anxiety in pregnancy. However, in terms of inducing labour, robust clinical trials are lacking, and it is not yet an established method for inducing labour. There is also no guidance provided by NICE or RCOG related to reflexology.
Primrose oil
The vaginal use of evening primrose oil could be considered as a safe and efficient approach for cervical ripening in low‐risk term pregnant women. The results of a systematic review showed that evening primrose oil could significantly improve the Bishop score. It is believed that gama-linoleic acid in evening primrose oil facilitates the making of prostaglandin and that prostaglandins play the most important role in the process of cervical ripening, as determined by Bishop score.
There is some evidence suggesting that evening primrose oil improves cervical ripening when compared with a placebo or with usual induction medication.
However, NICE and RCOG guidelines do not provide guidance on the use of evening primrose oil for induction of labour.
Eating 6 dates a day
Consumption of dates may decrease the need for induction of labour and shorten the length of the latent phase of labour. The theory is that date fruit is high in saturated and unsaturated fatty acids which may contribute to the production of prostaglandins needed for cervical ripening and labour. The high sugar content provides nutritional value during labour, but caution is advised amongst those with diabetes mellitus (gestational, type 1 or type 2). There is low-quality evidence to support the consumption of dates for induction of labour.
Fresh pineapple
Historically, pineapple is reputed to act as a means of inducing labour to avoid medical intervention of post-dates pregnancy.
Several reports and studies have claimed labour-induing qualities of pineapple fruit (ripe or unripe) in many parts of the world. Some research studies have indicated that pineapple has some potential effects on uterine contractions, which could theoretically be related to labour induction. However, these studies were conducted in a laboratory setting therefore do not translate to clinical significance for induction of labour in humans.
NICE or RCOG does not include any guidance on eating fresh pineapple for induction of labour.
References for options for starting and methods of inducing labour:
National Institute for Health and Care Excellence: Inducing labour [NG207] [Internet]. NICE, London; 2021 [cited 2024 Aug 14]. Available from: https://www.nice.org.uk/guidance/ng207
Hofmeyr GJ, Gülmezoglu AM, Pileggi C. Vaginal misoprostol for cervical ripening and induction of labour. Cochrane Database of Systematic Reviews 2010, Issue 10. Art. No.: CD000941. DOI: 10.1002/14651858.CD000941.pub2
Kerr RS, Kumar N, Williams MJ, Cuthbert A, Aflaifel N, Haas DM, Weeks AD. Low‐dose oral misoprostol for induction of labour. Cochrane Database of Systematic Reviews 2021, Issue 6. Art. No.: CD014484. DOI: 10.1002/14651858.CD014484
Rattanakanokchai S, Gallos ID, Kietpeerakool C, Eamudomkarn N, Alfirevic Z, Oladapo OT, et al. Methods of induction of labour: a network meta-analysis. Cochrane Pregnancy and Childbirth Group, editor. Cochrane Database Syst Rev [Internet]. 2023 Jan 3 [cited 2024 Aug 15];2023(1). Available from: http://doi.wiley.com/10.1002/14651858.CD015234
De Vaan MD, Ten Eikelder ML, Jozwiak M, Palmer KR, Davies-Tuck M, Bloemenkamp KW, et al. Mechanical methods for induction of labour. Cochrane Pregnancy and Childbirth Group, editor. Cochrane Database Syst Rev [Internet]. 2023 Mar 30 [cited 2024 Aug 15];2023(7). Available from: http://doi.wiley.com/10.1002/14651858.CD001233.pub4
Recommendations: Intrapartum care: Guidance 1.8.40 to 1.8.42. NICE. Available at: https://www.nice.org.uk/guidance/ng207/chapter/recommendations
Smyth RMD, Markham C, Dowswell T. Amniotomy for shortening spontaneous labour. Cochrane Database of Systematic Reviews 2013, Issue 6. Art. No.: CD006167. DOI: 10.1002/14651858.CD006167.pub4
Leathersich SJ, Vogel JP, Tran TS, Hofmeyr GJ. Acute tocolysis for uterine tachysystole or suspected fetal distress. Cochrane Database of Systematic Reviews 2018, Issue 7. Art. No.: CD009770. DOI: 10.1002/14651858.CD009770.pub2
References for alternative therapies:
National Institute for Health and Care Excellence: Guidelines. Inducing labour. London: National Institute for Health and Care Excellence (NICE) Copyright © NICE 2021.; 2021.
Zamawe C, King C, Jennings HM, Mandiwa C, Fottrell E. Effectiveness and safety of herbal medicines for induction of labour: a systematic review and meta-analysis. BMJ Open. 2018;8(10):e022499.
Smith CA, Armour M, Dahlen HG. Acupuncture or acupressure for induction of labour. Cochrane Database of Systematic Reviews. 2017(10).
Harper TC, Coeytaux RR, Chen W, Campbell K, Kaufman JS, Moise KJ, et al. A randomized controlled trial of acupuncture for initiation of labor in nulliparous women. J Matern Fetal Neonatal Med. 2006;19(8):465-70.
Smith CA. Homoeopathy for induction of labour. Cochrane Database Syst Rev. 2001;2003(4):Cd003399.
Kelly AJ, Kavanagh J, Thomas J. Castor oil, bath and/or enema for cervical priming and induction of labour. Cochrane Database of Systematic Reviews. 2013(7).
Azhari S, Pirdadeh S, Lotfalizadeh M, Shakeri MT. Evaluation of the effect of castor oil on initiating labor in term pregnancy. Saudi Med J. 2006;27(7):1011-4.
Kavanagh J, Kelly AJ, Thomas J. Sexual intercourse for cervical ripening and induction of labour. Cochrane Database Syst Rev. 2001;2001(2):Cd003093.
Amico JA, Finley BE. Breast stimulation in cycling women, pregnant women and a woman with induced lactation: pattern of release of oxytocin, prolactin and luteinizing hormone. Clin Endocrinol (Oxf). 1986;25(2):97-106.
Christensson K, Nilsson BA, Stock S, Matthiesen AS, Uvnäs-Moberg K. Effect of nipple stimulation on uterine activity and on plasma levels of oxytocin in full term, healthy, pregnant women. Acta Obstet Gynecol Scand. 1989;68(3):205-10.
Kavanagh J, Kelly AJ, Thomas J. Breast stimulation for cervical ripening and induction of labour. Cochrane Database of Systematic Reviews. 2005(3).
Nishi D, Shirakawa MN, Ota E, Hanada N, Mori R. Hypnosis for induction of labour. Cochrane Database of Systematic Reviews. 2014(8).
Bowman R, Taylor J, Muggleton S, Davis D. Biophysical effects, safety and efficacy of raspberry leaf use in pregnancy: a systematic integrative review. BMC Complementary Medicine and Therapies. 2021;21(1):56.
Tabatabaeichehr M, Mortazavi H. The Effectiveness of Aromatherapy in the Management of Labor Pain and Anxiety: A Systematic Review. Ethiop J Health Sci. 2020;30(3):449-58.
Smith CA, Collins CT, Crowther CA. Aromatherapy for pain management in labour. Cochrane Database of Systematic Reviews. 2011(7).
Spinnewijn WEM, Lotgering FK, Struijk PC, Wallenburg HCS. Fetal heart rate and uterine contractility during maternal exercise at term. American Journal of Obstetrics & Gynecology. 1996;174(1):43-8.
Watkins VY, O'Donnell CM, Perez M, Zhao P, England S, Carter EB, et al. The impact of physical activity during pregnancy on labor and delivery. Am J Obstet Gynecol. 2021;225(4):437.e1-.e8.
Shojaei B, Loripoor M, Sheikhfathollahi M, Aminzadeh F. The effect of walking during late pregnancy on the outcomes of labor and delivery: A randomized clinical trial. J Educ Health Promot. 2021;10:277.
Yayla Abide Ç, Kurek Eken M, Ozkaya E, Yenidede I, Bostanci Ergen E, Kilicci C, et al. Effect of vaginal washing before intravaginal dinoprostone insertion for labor induction: A randomized clinical trial. J Obstet Gynaecol Res. 2018;44(12):2149-55.
Verma ML, Pandey M, Singh U, Sachan R, Sankhwar PL. Effect of vaginal douching with normal saline before insertion of dinoprostone vaginal insert for labor induction. J Family Med Prim Care. 2024;13(1):265-70.
Smith CA, Collins CT, Cyna AM, Crowther CA. Complementary and alternative therapies for pain management in labour. Cochrane Database Syst Rev. 2006;2006(4):Cd003521.
Ernst E, and Köder K. An overview of reflexology. European Journal of General Practice. 1997;3(2):52-7.
Dolatian M, Hasanpour A, Montazeri S, Heshmat R, Alavi Majd H. The effect of reflexology on pain intensity and duration of labor on primiparas. Iran Red Crescent Med J. 2011;13(7):475-9.
Liang X, Wu S, Li K, Zhang H, Yang F, Wang X, et al. The effects of reflexology on symptoms in pregnancy: A systematic review of randomized controlled trials. Heliyon. 2023;9(8):e18442.
Ariana S, Amjadi N, Kazemi SN, Ahmadli Z. The Use of Evening Primrose Oil for Cervical Ripening in Low-Risk Women with Term Pregnancy: A Randomized Double-Blinded Controlled Trial. Complement Med Res. 2024;31(3):215-21.
Shahinfar S, Abedi P, Jahanfar S, Khajehpoor M, Chashmyazdan M. The effect of evening primrose oil on cervical ripening and birth outcomes: A systematic review and meta-analysis. Heliyon. 2023;9(2):e13414.
Bahmani S, Shahoei R. The effect of misoprostol with and without evening primrose oil on labor progress and neonatal Apgar score in post-term pregnancies: a clinical trial study. The Iranian Journal of Obstetrics, Gynecology and Infertility. 2023;26(3):43-52.
Azad A, Pourtaheri M, Darsareh F, Heidari S, Mehrnoush V. Evening primrose oil for cervical ripening prior to labor induction in post-term pregnancies: A randomized controlled trial. European Journal of Integrative Medicine. 2022;51:102123.
Sagi-Dain L, Sagi S. The effect of late pregnancy date fruit consumption on delivery progress - A meta-analysis. Explore (NY). 2021;17(6):569-73.
Al-Kuran O, L. A-M, H. B, S. B, and Amarin Z. The effect of late pregnancy consumption of date fruit on labour and delivery. Journal of Obstetrics and Gynaecology. 2011;31(1):29-31.
Monji F, Adaikan PG, Lau LC, Bin Said B, Gong Y, Tan HM, et al. Investigation of uterotonic properties of Ananas comosus extracts. Journal of Ethnopharmacology. 2016;193:21-9.
Monji F, Adaikan PG, Lau LC, Siddiquee AA, Said BB, Yang LK, et al. Role of the serotonergic pathway in uterotonic activity of Ananas comosus (L.) Merr. - An in vitro and in vivo study. Phytomedicine. 2018;48:32-42.