What to expect during induction
Pain relief during induction
Medical pain relief options
Tablets: Paracetamol and/or dihydrocodeine.
Paracetamol is a very commonly used pain relief medication. provides pain relief for mild-moderate pain. It can be given by mouth (orally) or by a drip in a vein in your arm (intravenously). It may provide some relief in the early stages of labour. Paracetamol takes about an hour to take effect and provides relief for 4-6 hours.
Dihydrocodeine is also commonly used in labour for moderate pain. It is recommended over codeine due to evidence on its safety. It is given by mouth (orally). Dihydrocodeine takes about an hour to take effect and provides relief for 4-6 hours.
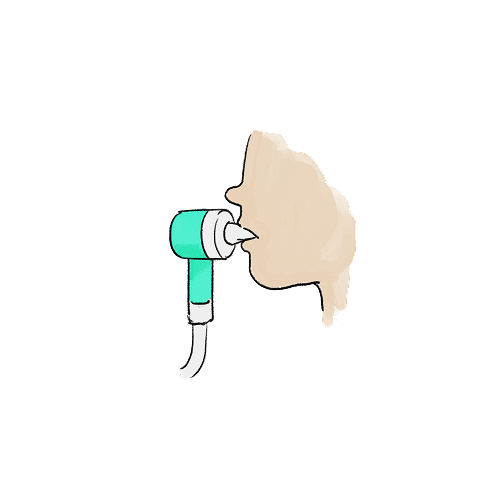
Gas & air (Entonox) is the most common pain relief in labour. Entonox is a mixture of 50% oxygen and 50% nitrous oxide gas that you breathe in via a mouthpiece or facemask when you need it. You are in control the amount of Entonox you use, but to get the best effect it is important to get the timing right. You should start breathing Entonox as soon as you feel a contraction coming on to get the full effect when the contraction is at its peak. You should then stop using Entonox as the contraction ends, breathing normal air between your contractions. It works quickly and wears off in a few minutes making you feel more relaxed, but it does not take away the pain completely. It has no harmful effects on your baby and can be used at any stage in labour. Entonox is safe to use, and common side effects include a dry mouth, feeling sick (nausea) and vomiting, and feeling dizzy, light-headed or sleepy. The side effects are mild and go away as you stop using Entonox.
Injections, such as opioids, pethidine, and diamorphine are strong pain-relieving medicines that can be given by an injection into your muscle in your thigh (intramuscular). It starts to work about half an hour after the injection and can last for a few hours. Opioids can make you and your baby feel sleepy or develop a short-term respiratory depression, so there is a chance that your baby may need some extra support when they are born. They also can make you feel sick, but you can be given anti-sickness medicine for it. High doses of opioids can slow down your breathing, this is very rare with the doses given in labour.
Epidural is a type of spinal injection to stop you feeling pain in the lower half of your body, typically where your contractions are. Epidurals can be the most effective method of pain relief for labour. The anaesthetist will insert a needle into the lower part of your back and use it to place a very thin tube (epidural catheter) near the nerves in your spine. The epidural catheter is left in place when the needle is taken out so you can be given painkillers through it during your labour. The painkillers may be a local anaesthetic to numb your nerves, small doses of opioids, or a mixture of both. It may take 40 minutes to work to give pain relief. An epidural should not make you feel drowsy or sick. An epidural will have a very little effect on your baby but there may be an increased chance your obstetrician will need to use a ventouse (suction cup on your baby’s head) or forceps to deliver the baby (instrumental birth).

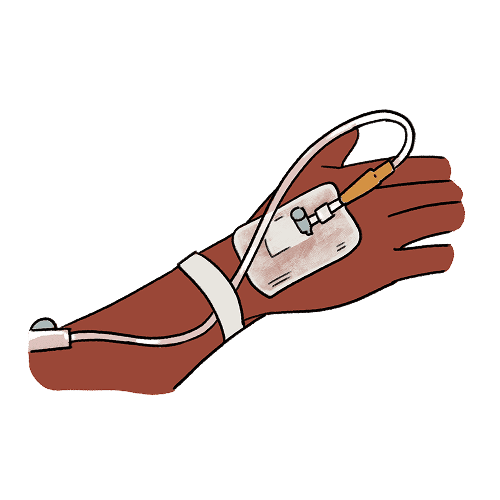
Patient-controlled intravenous analgesia (PCA) is a method of pain relief where you can give yourself (self-administer) opioid drugs using a pump attached to a drip. The medicines used for PCA are remifentanil or fentanyl. The medicines used for PCA act quickly but only for a short time. This makes them a good choice to help with the pain of contractions. It may not be as effective as epidural; therefore, it may be possible to combine PCA with gas & air. Side effects may include slowed breathing, reduced oxygen levels, itchiness, feeling sick or sleepy, but these medicines have very little effect on your baby. These problems are easy to treat but it means that you will be closely monitored and may need some oxygen. If there are any concerns that it is no longer safe to use a PCA, the anaesthetic team will explain this to you and offer alternative pain relief options.
Non-medical pain relief options
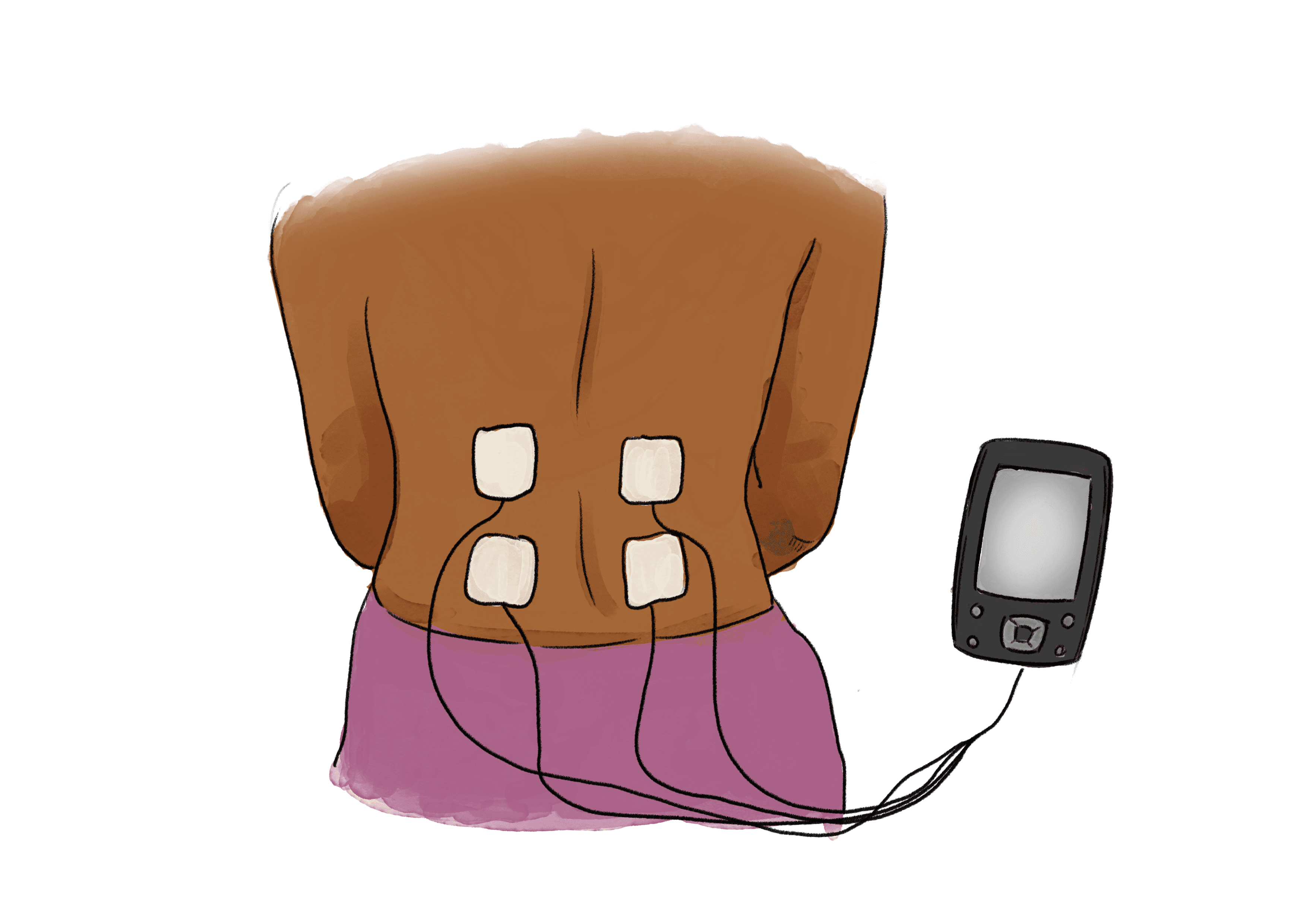
Transcutaneous electrical nerve stimulation (TENS) machine is a method of pain relief involving the use of a mild electrical current. It has no harmful effects on your baby. A gentle electrical current is passed through four flat pads stuck to your back, creating a tingling feeling. You can control the strength of the current yourself. It is sometimes helpful at the beginning of labour, particularly for backache. It is common to need some other pain relief later in labour. TENS devices are not provided by the NHS, but you can bring you own with you for your labour.
Studies have shown that water birth was found to be less painful, and you will be less likely to need an epidural to reduce the pain. It does not add any risks to you or your baby, and your midwife will regularly check the temperature of the water to check it is safe and not rising above 37.5°C. There are certain situations where it is not possible to have a water birth and access to pools are limited in maternity units, talk to your team about your options.
Sterile water injection can be used as a pain relief option for back pain. Water injections can provide relief of back pain from 10 minutes after the injection for up to 3 hours. It can cause an initial stinging sensation.
Breathing exercise, having a shower or bath, and massage may reduce pain during the latent first stage of labour.
References:
Bisson DL, Newell SD, Laxton C, on behalf of the Royal College of Obstetricians and Gynaecologists. Antenatal and Postnatal Analgesia. Scientific Impact Paper No. 59. BJOG 2019; 126: e115–24
Othman M, Jones L, Neilson JP. Non‐opioid drugs for pain management in labour. Cochrane Database of Systematic Reviews 2012, Issue 7. Art. No.: CD009223. DOI: 10.1002/14651858.CD009223.pub2. Accessed 17 March 2025.
Middleton P, Shepherd E, Morris J, Crowther CA, Gomersall JC. Induction of labour at or beyond 37 weeks' gestation. Cochrane Database of Systematic Reviews 2020, Issue 7. Art. No.: CD004945. DOI: 10.1002/14651858.CD004945.pub5. Accessed 18 March 2025.
Entonox. LabourPains.com. Accessed August 13, 2024.https://www.labourpains.org/during-labour/gas-and-air
Opioids. LabourPains.com. Accessed August 13, 2024.https://www.labourpains.org/during-labour/opioids
Epidural analgesia. LabourPains.com. Accessed August 13, 2024.https://www.labourpains.org/during-labour/epidural-advice-and-information
Patient-controlled intravenous analgesia. LabourPains.com. Accessed August 18, 2024.https://www.labourpains.org/during-labour/patient-controlled-intravenous-analgesia
TENS machine. LabourPains.com. Accessed August 18, 2024.https://www.labourpains.org/during-labour/tens-machine
Water birth. LabourPains.com. Accessed August 19, 2024.https://www.labourpains.org/during-labour/water-pool
Intrapartum care. 1.6 Pain relief during labour. NICE guidelines. Published September 29, 2023. Accessed August 19, 2024.https://www.nice.org.uk/guidance/NG235/chapter/recommendations#pain-relief-during-labour
Inducing labour. 1.5 Assessment before induction, monitoring and pain relief. Published November 4, 2021. Accessed August 19, 2024.https://www.nice.org.uk/guidance/ng207/chapter/Recommendations#assessment-before-induction-monitoring-and-pain-relief