Monitoring, interventions and procedures
Possible procedures or interventions during labour
Methods to reduce the risk of serious tears to the perineum:
There are different types of tears which can happen during childbirth, some heal by themselves and others need stitches.
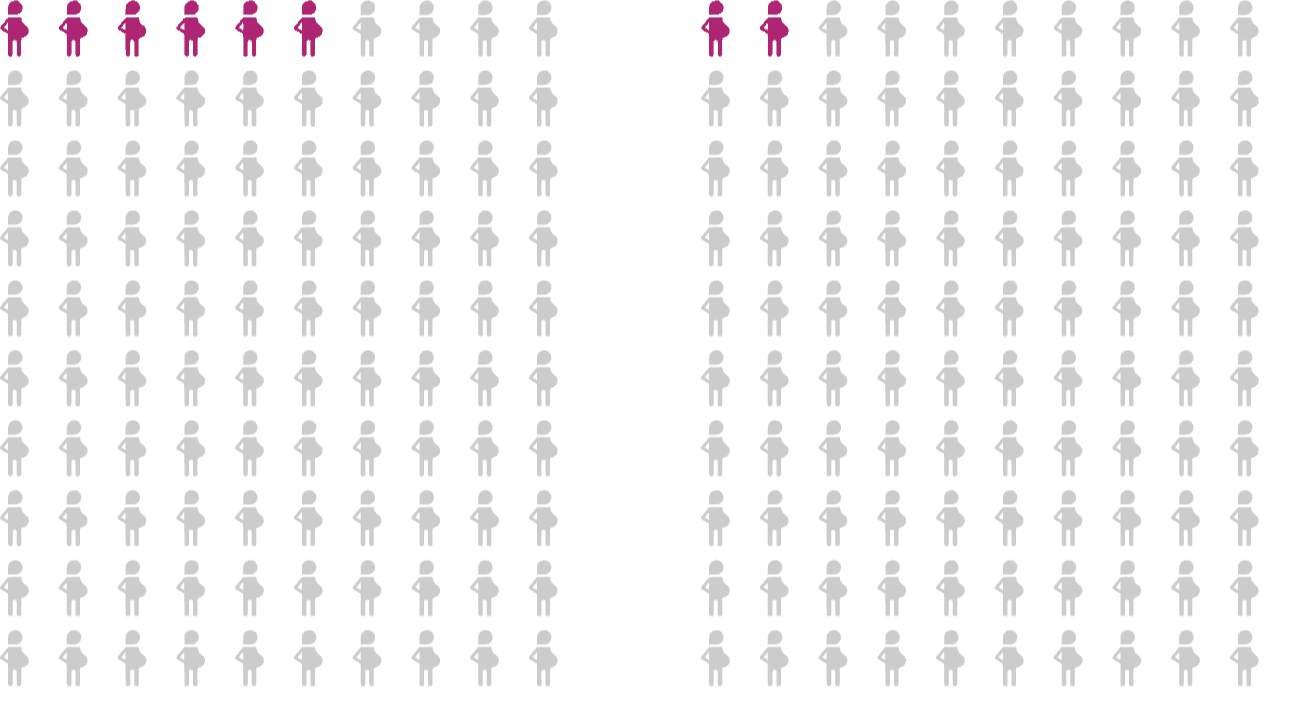
The more serious tears, the ones which include the anus, and can mean difficulties in holding in poo or wind, happen in around 6 in 100 of first births and around 2 in 100 subsequent births. Your midwife/doctor can try preventing these in multiple ways.
Guided Pushing: This is where your midwife will tell you when to push/or not. You may be instructed to take a deep breath at the start of the contraction and then push through the contraction. You may also be advised to puff or pant when your baby’s head is visible. These are both methods to help reduce the risk of a more serious tear. This guided pushing can also reduce the likelihood of needing an assisted birth which increases your risk of a more serious tear to the vagina.
Massage/Warm Compress: holding a warm compress on your perineum (the area between your vagina and your back passage) or massage your perineum with water soluble lubricant during the time you are pushing.
Guiding your baby’s head out whilst supporting the perineum at the time of the baby’s head being born can help reduce the risk of a more serious tear.
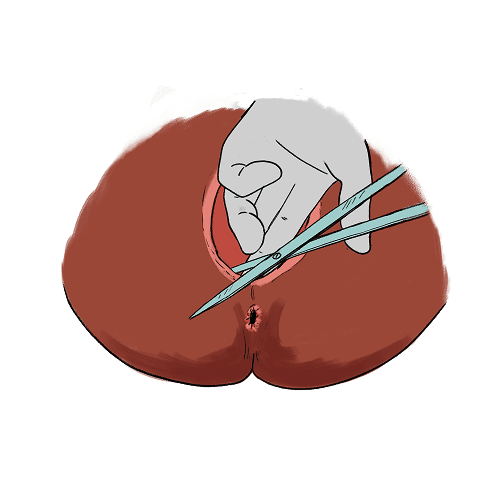
Episiotomy: A small cut to the perineum. You may be offered this if your baby needs extra room to be born, and your midwife or doctor feel that a more serious tear is likely and are trying to reduce this risk. This is more likely to be considered during an instrumental vaginal birth or if your midwife/doctor suspects that your baby is not getting enough oxygen and needs to be born quickly.
When an episiotomy may be offered
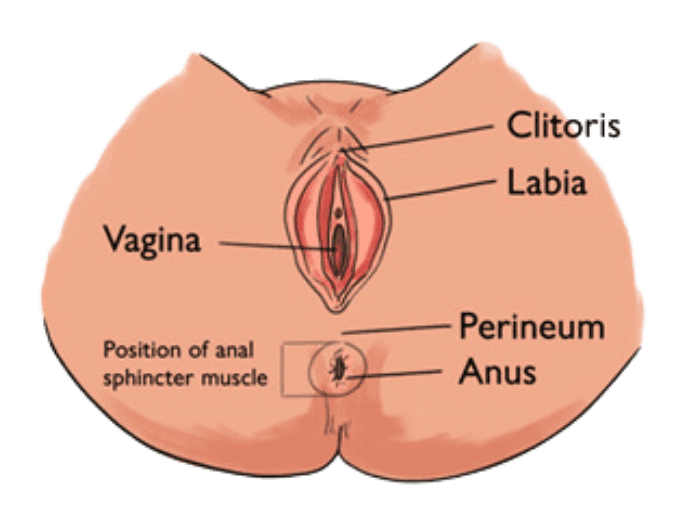
An episiotomy is a small cut made at the opening of the vagina at the time of birth.
During labour, an episiotomy may be recommended to you. An episiotomy will only be offered to you if your midwife or doctor feels that there is a risk of a more serious perineal tear, or the birth of your baby is very urgent. This may be necessary during an instrumental vaginal birth
An episiotomy is a cut which is made at the opening of the vagina into the perineum to give you baby more room to be born. The aim of an episiotomy is to reduce the seriousness of a perineal tear or to birth you baby as quickly as possible.
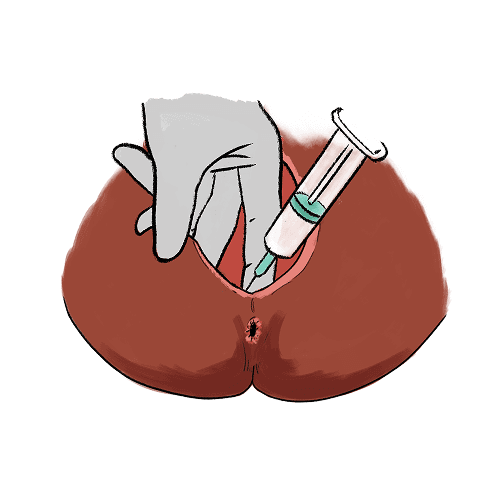
If you accept the episiotomy, you will usually be numbed using local anaesthetic and you will require some stitches afterwards. This may happen in your labour room or in a surgical theatre, this would be discussed with you and the reasons for the choice of location.
When an Instrumental or caesarean birth may be offered or recommended and why.
There are multiple different ways to give birth.
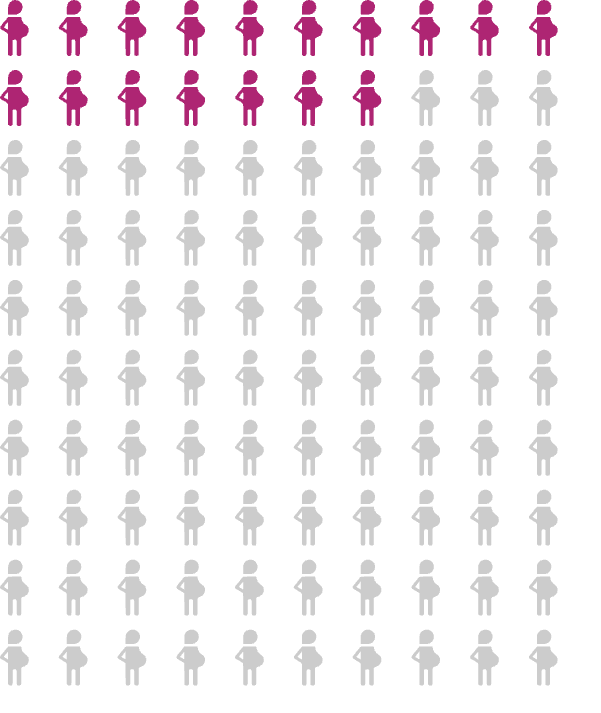
Around 17 in 100 women experience instrumental vaginal birth during their first birth, and 6 in 100 during subsequent births.
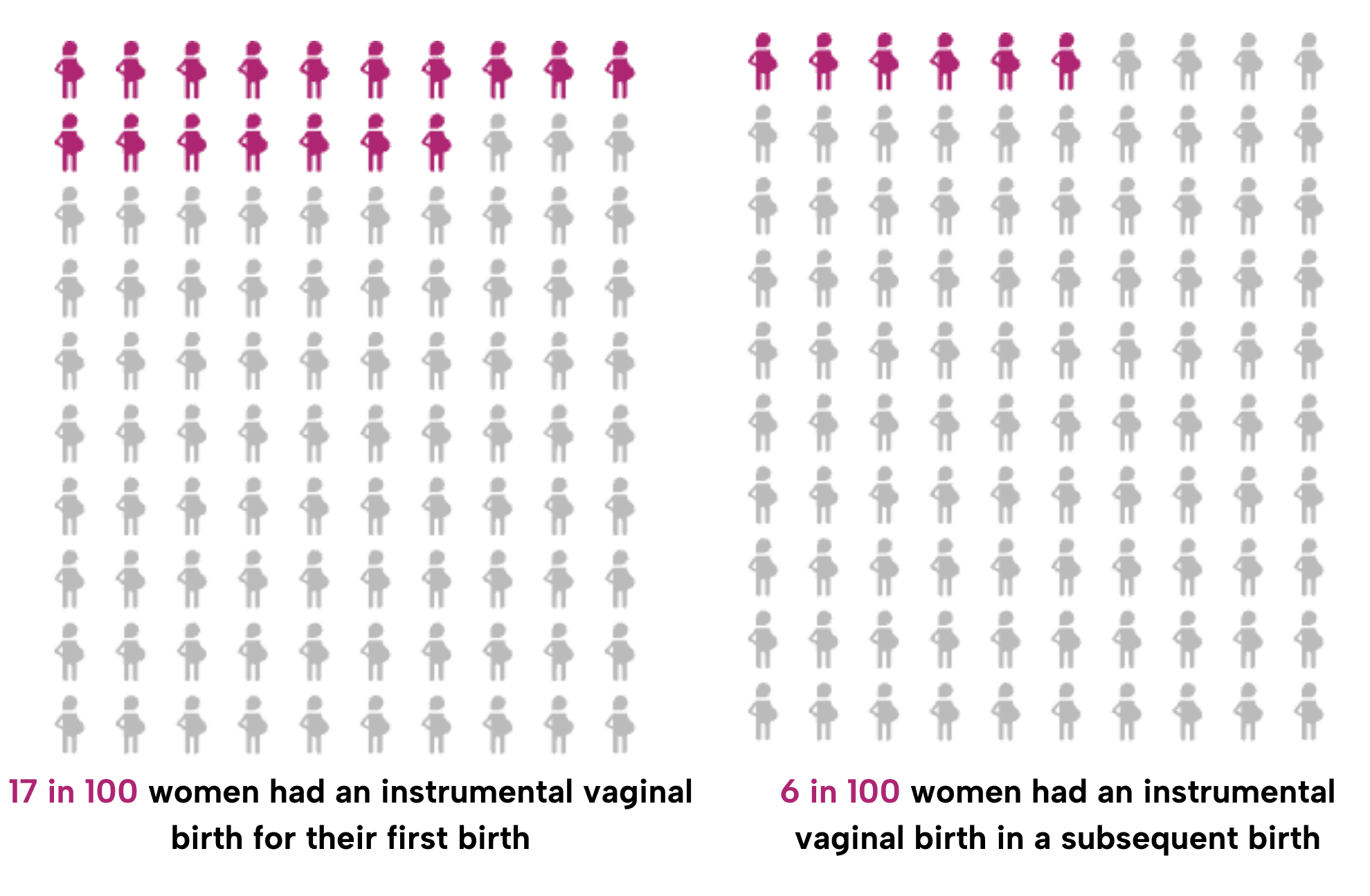
This can be due to delay during the second stage, maternal request or concerns that your baby is getting enough oxygen.
There are two main types of instruments which can be used. One is called forceps and these are like big metal spoons.
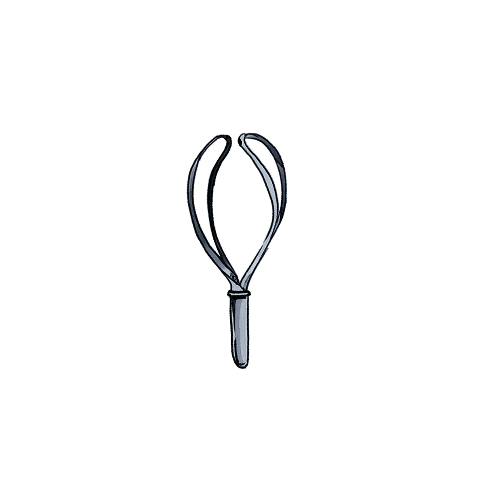

The other type of is a suction cup (ventouse), these instruments are put on your baby’s head to help guide them out whilst you are pushing.

Sometimes you will be offered an episiotomy to reduce risk of tears to your perineum because it is more likely you will have a more serious perineal tear when having an instrumental birth. This happens in around 17 in 100 instrumental births.
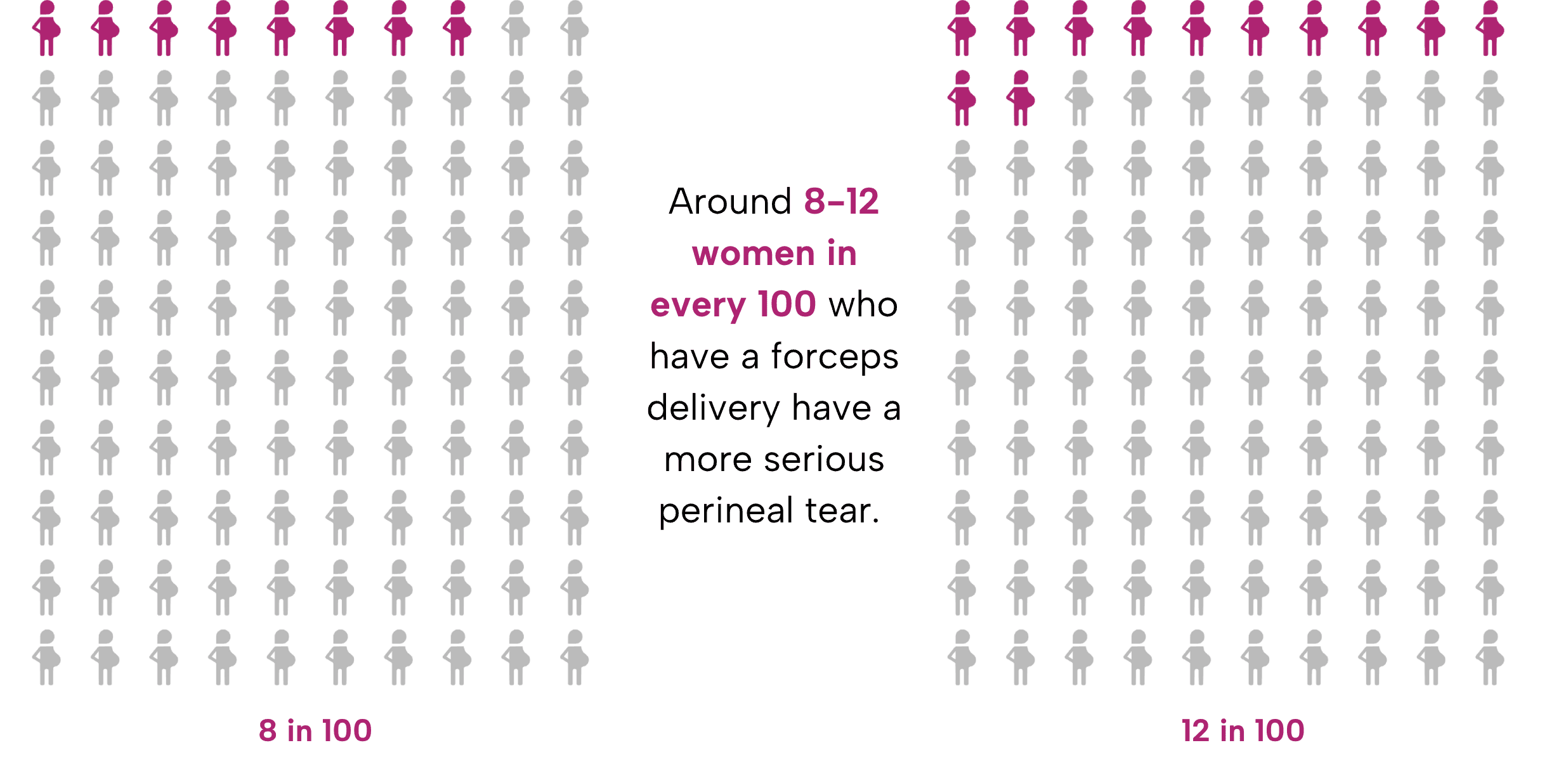
Around 8-12 women in every 100 who have a forceps delivery have a more serious perineal tear.
With a ventouse, sometimes the cup pops off and makes a sound and will need to be put back on, or there will need to be a switch to forceps.
Up to 4 in 100 women who deliver with a ventouse will have more serious perineal tear (3rd or 4th degree tear).

If it is not viable to try an instrumental birth or if it doesn’t work, a caesarean birth can be offered. A caesarean is where your baby is delivered through a cut to your abdomen and uterus. This is done in a surgical theatre with multiple doctors and your midwife present. You get an injection into your back to numb you from your chest to your toes so that you don’t feel pain when your abdomen is cut into.
When you are in the second stage it may well be faster and safer for your baby to be born by instrumental vaginal birth than an urgent caesarean birth. For example, if the baby’s head is too low, a caesarean birth is associated with difficulties in your baby’s head being born (known as impacted fetal head) and this can be associated with babies getting a lack of oxygen or having injuries during birth.
To read more about planned/unplanned or emergency caesarean birth click here.
Reducing risk of tear references:
Intrapartum care. NICE guidelines Published September 29, 2023. Accessed October 18, 2023. https://www.nice.org.uk/guidance/ng235/chapter/Recommendations#planning-place-of-birth
Episiotomy. Royal College of Obstetricians and Gynaecologists. https://www.rcog.org.uk/for-the-public/perineal-tears-and-episiotomies-in-childbirth/episiotomy/
Assisted vaginal birth (ventouse or forceps). Royal College of Obstetricians and Gynaecologists. https://www.rcog.org.uk/for-the-public/browse-our-patient-information/assisted-vaginal-birth-ventouse-or-forceps/
Fernado RJ, Sultan AH, et al on behalf of the Royal College of Obstetricians and Gynaecologists. The Management of Third-and-Fourth-Degree Perineal Tears. BJOG 2015
Episiotomy references:
Intrapartum care. NICE guidelines Published September 29, 2023. Accessed October 18, 2023. https://www.nice.org.uk/guidance/ng235/chapter/Recommendations#planning-place-of-birth
Episiotomy. Royal College of Obstetricians and Gynaecologists. https://www.rcog.org.uk/for-the-public/perineal-tears-and-episiotomies-in-childbirth/episiotomy/
Fernado RJ, Sultan AH, et al on behalf of the Royal College of Obstetricians and Gynaecologists. The Management of Third-and-Fourth-Degree Perineal Tears. BJOG 2015
Murphy DJ, Strachan BK, Bahl R, on behalf of the Royal College of Obstetricians Gynaecologists. Assisted Vaginal Birth. BJOG 2020;127:e70–e112.
Caesarean birth. NICE guidelines. Published March 31, 2021. Accessed October 20, 2023. https://www.nice.org.uk/guidance/ng192
Instrumental birth references:
NHS Maternity Statistics, England, 2023-24. last accessed 10/03/25. Available from: https://digital.nhs.uk/data-and-information/publications/statistical/nhs-maternity-statistics/2023-24/births
NMPA Project Team. National Maternity and Perinatal Audit: Clinical Report 2022. Based on births in NHS maternity services in England and Wales between 1 April 2018 and 31 March 2019. London: RCOG; 2022.
Intrapartum care. NICE guidelines Published September 29, 2023. Accessed October 18, 2023. https://www.nice.org.uk/guidance/ng235/chapter/Recommendations#planning-place-of-birth
Episiotomy. Royal College of Obstetricians and Gynaecologists. https://www.rcog.org.uk/for-the-public/perineal-tears-and-episiotomies-in-childbirth/episiotomy/
Assisted vaginal birth (ventouse or forceps). Royal College of Obstetricians and Gynaecologists. https://www.rcog.org.uk/for-the-public/browse-our-patient-information/assisted-vaginal-birth-ventouse-or-forceps/
Murphy DJ, Strachan BK, Bahl R, on behalf of the Royal College of Obstetricians Gynaecologists. Assisted Vaginal Birth. BJOG 2020;127:e70–e112.
Caesarean birth. NICE guidelines. Published March 31, 2021. Accessed October 20, 2023. https://www.nice.org.uk/guidance/ng192
Wyn Jones N, Mitchell EJ, Wakefield N, et al. Impacted fetal head during second stage Caesarean birth: A prospective observational study. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2022;272:77-81. doi:10.1016/j.ejogrb.2022.03.004
Perineal tears and episiotomy. NHS inform. Accessed December 4, 2023. https://www.nhsinform.scot/ready-steady-baby/labour-and-birth/assisted-birth/perineal-tears-and-episiotomy/