Possible benefits and risks
Risks for the mother
Risks at the time of the caesarean birth
Bleeding
Losing more than 500mls of blood during caesarean birth is very common: 31 in 100 women/birthing people.

Although bleeding is very common, bleeding requiring blood transfusion happens less frequently. The chance of needing a blood transfusion is: 3 in 100 women/birthing people. The chance of being offered a blood transfusion will depend on the amount of bleeding, your body size, your blood results, and how your body is coping. The risks and benefits of this will be discussed and iron tablets may also be recommended.
Your midwives and doctors will be used to treating bleeding after birth. They will work as a team to stop you bleeding and may need to give you an injection, put a tube into a vein for medicine, rub your womb and do a vaginal examination. Some women will need to go to the operating theatre to stop the bleeding. Emergency removal of the womb (hysterectomy)in order to to stop bleeding and save your life is uncommon: About 2 in 1000 women/birthing people.
Chance of injury to nearby organs

Injuries to your your bladder, the tubes connecting your kidney to your bladder (ureters) or bowel is uncommon, and happens in about 1 in 1,000 births. It may be more likely with multiple previous caesarean births, scar tissue from previous operations, past infections inside your womb or chronic conditions including endometriosis. Emergency Caesarean birth performed in the advanced stages of labour can also increase your likelihood of these injuries. If the doctor spots the injury at the time, they will try to fix it. Sometimes they do not see it at the time and it will be found at a later date.
Chance of death of mother
Maternal death happens in about 25 in 100,000 births. It can be due to developing clots in the lungs, significant bleeding, infection or existing or new medical problems.
There are also small risks with anaesthetics which you can read more about here.
Short term risks after a caesarean birth
Going back to theatre
Sometimes because of bleeding, infections or other problems. Another procedure may be necessary.
Reasons for needing to return to theatre include:
Bleeding that does not respond to medication and requires surgical management
A collection of blood under the skin or in your abdomen that need to be managed in theatre
Injuries that become apparent after caesarean birth, for example to your bladder or bowels, that need surgery to repair them.
Admission to critical care unit
Critical care, also known as intensive care, is specialist medical care for life-threatening complications of surgery or illness.
Admission to critical care is uncommon, occurs in 3 in 1000 births. This is higher than if you have a vaginal birth: 1 in 1,000 women/birthing people.
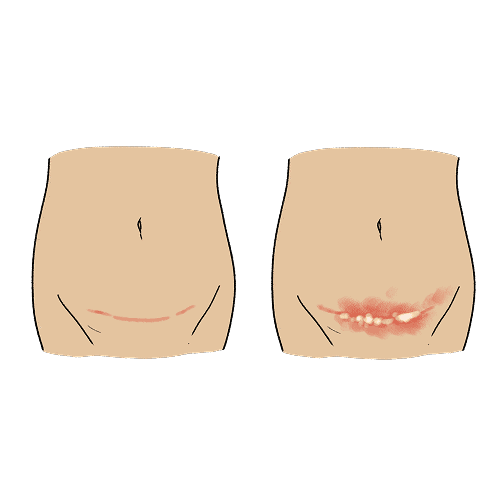
Wound Infection

If you have a body mass index (BMI) of 35 kg/m2 or more, to reduce the risk of wound infection you may be offered a specialist dressing to provide negative pressure wound therapy and promote healing.
If you have a standard dressing (not negative pressure) no particular type of wound dressing has been shown to be better than another to reduce the risk of infections.
There is no difference in the risk of wound infection when dressings are removed 6 or 24 hours post-operatively.
Your temperature will be monitored after your caesarean birth for signs of a fever. Other signs of infection to be aware of include increasing pain, redness or discharge.
You should wear loose, comfortable clothes and cotton underwear if possible.
You will have routinely received antibiotics (through a drip) at the time of surgery to reduce the likelihood of infection.
The chance of wound infection might increase following an emergency caesarean birth, if you have diabetes, a high body mass index, or other conditions or medications that affect your immunity.
Mental health
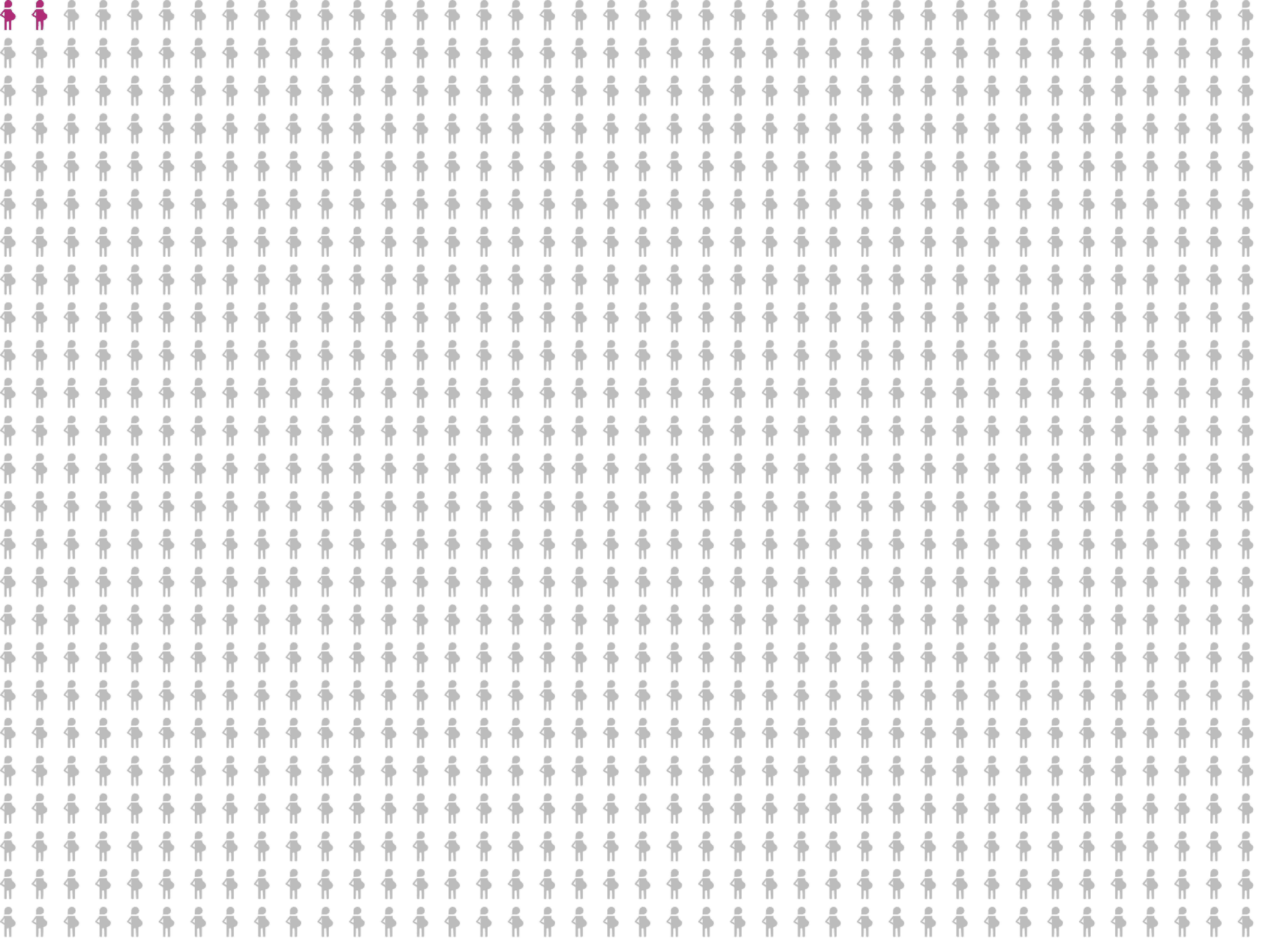
After a caesarean birth, psychological complications such as postnatal depression or post-traumatic stress disorder (PTSD) are common: 3 in 100 women/birthing people.
However, you are not at increased risk of depression or post-traumatic stress symptoms compared to women who have a spontaneous vaginal birth.
The likelihood of developing perinatal mental health problems is increased if you have experienced them in a previous pregnancy, have a mental health condition such as depression or bipolar disorder, have a family history of mental health disorders or experienced a traumatic birth.
Midwives, doctors or other health professionals will ask you how you are feeling after your birth and during the postnatal period. They can provide support to help you or refer you to more specialist services.
It affects 3 in 100 women/birthing people

Developing blood clots in legs and lungs

Pregnancy, birth and the postnatal period are times when the likelihood of developing blood clots in the legs and lungs (venous thromboembolism or VTE) is higher.
Pre-existing conditions that may increase your chance of a blood clot are if you, or a close family member, have had a previous blood clots, have certain medical conditions (thrombophilia, cancer, heart failure, diabetes) are above 35 years, have a body mass index over 30 in pre-pregnancy or in early pregnancy, smoke, have severe varicose veins or are paraplegic.
Risk factors associated with pregnancy include multiple pregnancy, current pre-eclampsia, labour longer than 24 hours, caesarean section, any type of operative delivery, stillbirth, preterm birth, and post-partum haemorrhage over 1,000 ml.
Some women receive treatment to prevent blood clots during pregnancy. If you are one of these women and you are having a planned caesarean you should follow the advice of your clinical team who will plan with you when to stop it.
National guidance also recommends all women having a caesarean birth are offered treatment to minimize their risk of VTE. Your individual risk will be assessed, you will be advised to remain hydrated and keep moving around. Most women and birthing people are offered graduated compression stockings, some are offered blood thinning injections (Low Molecular Weight Heparin).
Long term risks after a caesarean birth
Incontinence (leaking urine, faeces or wind)
Stress incontinence is when you leak urine (wee) when your bladder is under pressure during activities such as exercise, coughing, sneezing, or laughing. Following a caesarean birth about 4 in 100 of women will experience some stress incontinence.
Leaking urine (wee) more than a year after birth is common: 7-20 in 100.
Urinary incontinence can happen after you have a baby because of pressure during pregnancy, or injury during labour, or injuries to small nerves during a caesarean birth.
Leaking faeces (poo) or flatus (wind) more than a year after birth is common: 8 in 100 women/birthing people. This is more likely if you have an unplanned/emergency caesarean section during labour.
Pelvic Organ Prolapse - bulging bladder, womb or back passage (rectum)
Pelvic organ prolapse (bulging bladder, womb or back passage (rectum)) requiring hospital treatment after a year is uncommon: 2 in 1,000 women/birthing people.
Any pregnancy and birth can increase the likelihood of developing prolapse later in life, whether you had a vaginal or a caesarean birth.
References for short-term risks:
NHS Maternity Statistics, England, 2023-24. last accessed 10/03/25. Available from: https://digital.nhs.uk/data-andinformation/publications/statistical/nhs-maternity-statistics/2023-24/births
Khan KS, Moore PAS, Wilson MJ, Hooper R, Allard S, Wrench I, Beresford L, Roberts TE, McLoughlin C, Geoghegan J, Daniels JP, Catling S, Clark VA, Ayuk P, Robson S, Gao-Smith F, Hogg M, Lanz D, Dodds J; SALVO study group. Cell salvage and donor blood transfusion during cesarean section: A pragmatic, multicentre randomised controlled trial (SALVO). PLoS Med. 2017 Dec 19;14(12):e1002471. doi: 10.1371/journal.pmed.1002471
Royal College of Obstetricians and Gynaecologists. Planned Caesarean Birth: Consent Advice No. 14 August 2022 Minor Update November 2024
Larsson C, Djuvfelt E, Lindam A, Tunón K, Nordin P. Surgical complications after caesarean section: A population-based cohort study. PLoS One. 2021 Oct 5;16(10):e0258222. doi:10.1371/journal.pone.0258222
References for long-term risks:
Royal College of Obstetricians and Gynaecologists. Planned Caesarean Birth: Consent Advice No. 14 August 2022 Minor Update November 2024.
Larsson C, Källen K, Andolf E. Cesarean section and risk of pelvic organ prolapse: a nested case-control study. Am J Obstet Gynecol. 2009 Mar;200(3):243.e1-4. doi: 10.1016/j.ajog.2008.11.028.
Rowlands, I.J., Redshaw, M. Mode of birth and women’s psychological and physical wellbeing in the postnatal period. BMC Pregnancy Childbirth 12, 138 (2012). https://doi.org/10.1186/1471-2393-12-138.
Reducing the Risk of Thrombosis and Embolism during Pregnancy and the Puerperium (Green-top Guideline No. 37a). Accessed 10/03/2025. Available from: https://www.rcog.org.uk/guidance/browse-all-guidance/greentop-guidelines/reducing-the-risk-of-thrombosis-and-embolismduring-pregnancy-and-the-puerperium-green-top-guideline-no-37a/.
Herstad L, Klungsøyr K, Skjærven R, Tanbo T, Forsén L, Åbyholm T, Vangen S. Elective cesarean section or not? Maternal age and risk of adverse outcomes at term: a population-based registry study of low-risk primiparous women. BMC Pregnancy Childbirth. 2016 Aug 17;16:230. DOI: 10.1186/s12884-016-1028-3.