Supporting you to make a decision
Risks of induction of labour
Key considerations for mothers
Key considerations for mothers

Induction of labour is a medical intervention that will affect your birth options including:
Vaginal examinations to assess the cervix are needed before and during induction, to determine the best method of induction and to monitor progress.
Your choice of place of birth will be limited, as you may be recommended interventions (for example, oxytocin infusion, continuous fetal heart rate monitoring and epidurals) that are not available for home birth or in midwife-led birth units. There may be limitations on the use of a birthing pool.
There may be a need for an instrumental birth (using forceps or ventouse), with its increased risk of severe perineal tears (third- or fourth-degree perineal tears) but there is evidence that this is not increased in comparison to if you wait for spontaneous labour.
An induced labour may be more painful than a spontaneous labour.
Your hospital stay may be longer than with a spontaneous labour.
If you have an outpatient induction, we won’t monitor you and your baby as frequently as you would be if you were an inpatient. This includes your observations and monitoring baby’s heart rate therefore there’s a small chance of us not detecting a problem with you or your baby’s vital signs while you’re at home.
There is a chance that you may not go into active labour.
Possible risks for the mother with induction of labour
If your labour is longer than usual, or your waters have been broken early in the induction, there may be a higher chance of you developing an infection in your womb (chorioamnionitis).
The different risks associated with cervical ripening.
Membrane sweeping can cause pain, discomfort and vaginal bleeding.
Using medication to start your induction can cause hyperstimulation – this is when the uterus contracts too frequently or contractions last too long, which can lead to changes in fetal heart rate and result in fetal distress. Speak to your local maternity unit about which medications they plan to use to induce your labour.
Mechanical methods of ripening your cervix carry a small risk of infection, not supported by strong evidence.
The different risks associated with induction of contractions
Using oxytocin to increase the frequency and strength of your contractions can cause hyperstimulation – this is when the uterus contracts too frequently or last too long, which can lead to changes in fetal heart rate and result in fetal distress.
Once your waters are broken (amniotomy), you can choose to commence oxytocin immediately, delay starting this or can choose not to have it at all. Delaying or choosing not to use oxytocin may mean that your labour takes longer, and there may be an increased risk of infection in your baby.
Possible risks with induction of labour for the baby
Using oxytocin to increase the frequency and strength of your contractions can cause hyperstimulation – this is when the uterus contracts too frequently or lasts too long, which can lead to changes in fetal heart rate and result in fetal distress.
We will monitor your baby’s heartrate using a CTG. This way of monitoring your baby detects changes in the pattern of their heartrate over time. Occasionally the pattern can look clinically suspicious, and your midwife may need to monitor you more closely, change your position or ask for a specialist doctor to review you.
Specifically important risk or emergency situations
Specifically important risk situations
Previous caesarean birth:
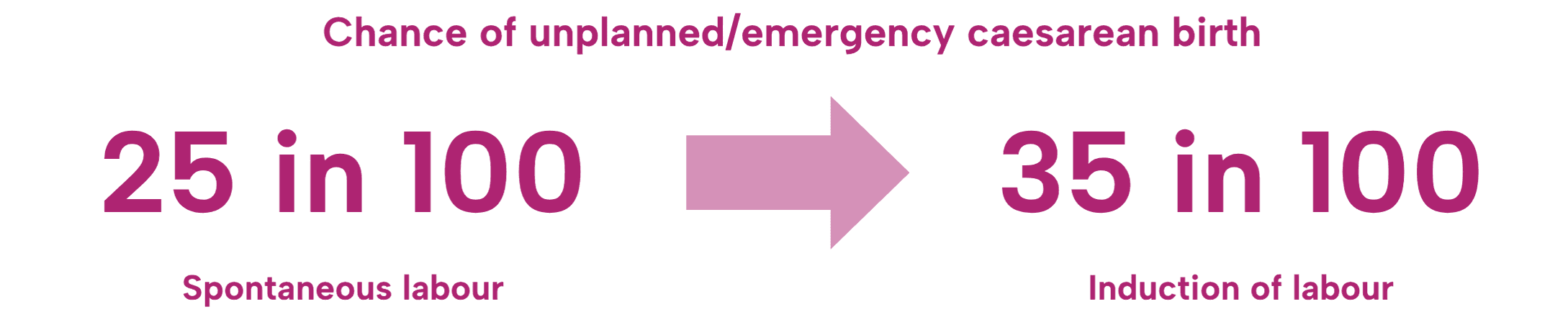
Induction of labour increases your chance of unplanned or emergency caesarean section compared with those that have physiological labour without induction or use of oxytocin to increase your contraction frequency in labour.
Induction of labour can increase your risk of uterine rupture 2-3-fold compared with those that have physiological labour without induction or use of oxytocin to increase your contraction frequency in labour.

Large for gestational age baby:
There is an increased risk of third- or fourth-degree perineal tears with induction of labour compared to physiological birth. There may be a higher chance that your baby will need phototherapy (light therapy) for jaundice (raised bilirubin levels).
Small for gestational age baby/gestational diabetes, pregnancy induced hypertension/pre-eclampsia:
If you undergo induction earlier than 39 weeks (37-38+6 weeks):
There is an increased chance that your baby will need to go to the neonatal unit.
Possible longer-term risk of special educational needs.
Maternal BMI 30kg/m2 or greater (Obesity):
Overall, you have increased chances of the events below occurring during your labour:
Caesarean section.
Pain relief requirements.
Shoulder dystocia.
Postpartum haemorrhage.
Possible delays during the process of induction:
Your induction of labour may be delayed depending on the clinical demand in your unit. Your maternity unit will only commence your induction of labour when there is enough staff to take care of you and there are not too many emergencies. If this happens, the staff will prioritise the scheduled inductions according to their clinical urgency. For more information, please contact your maternity unit leading up to your induction.
Once you have undergone cervical ripening, there may be a delay transferring you to the delivery suite to have your waters broken (amniotomy). Your unit must ensure that they have a midwife to take care of you during your labour. Sometimes you may have to wait for a midwife to become available to care for you safely.
Once you have given birth, there may be a delay transferring you to the maternity ward for postnatal care. You may be required to wait until a bed is available after other women/birthing people have been discharged.
There may be a wait for you to be discharged. Your midwife may be taking care of several women/birthing people at the same time and have several tasks to complete. Your midwife will prioritise their tasks depending on the clinical demands on the day. You may also be required to wait for your discharge medication from pharmacy.
Cord-prolapse
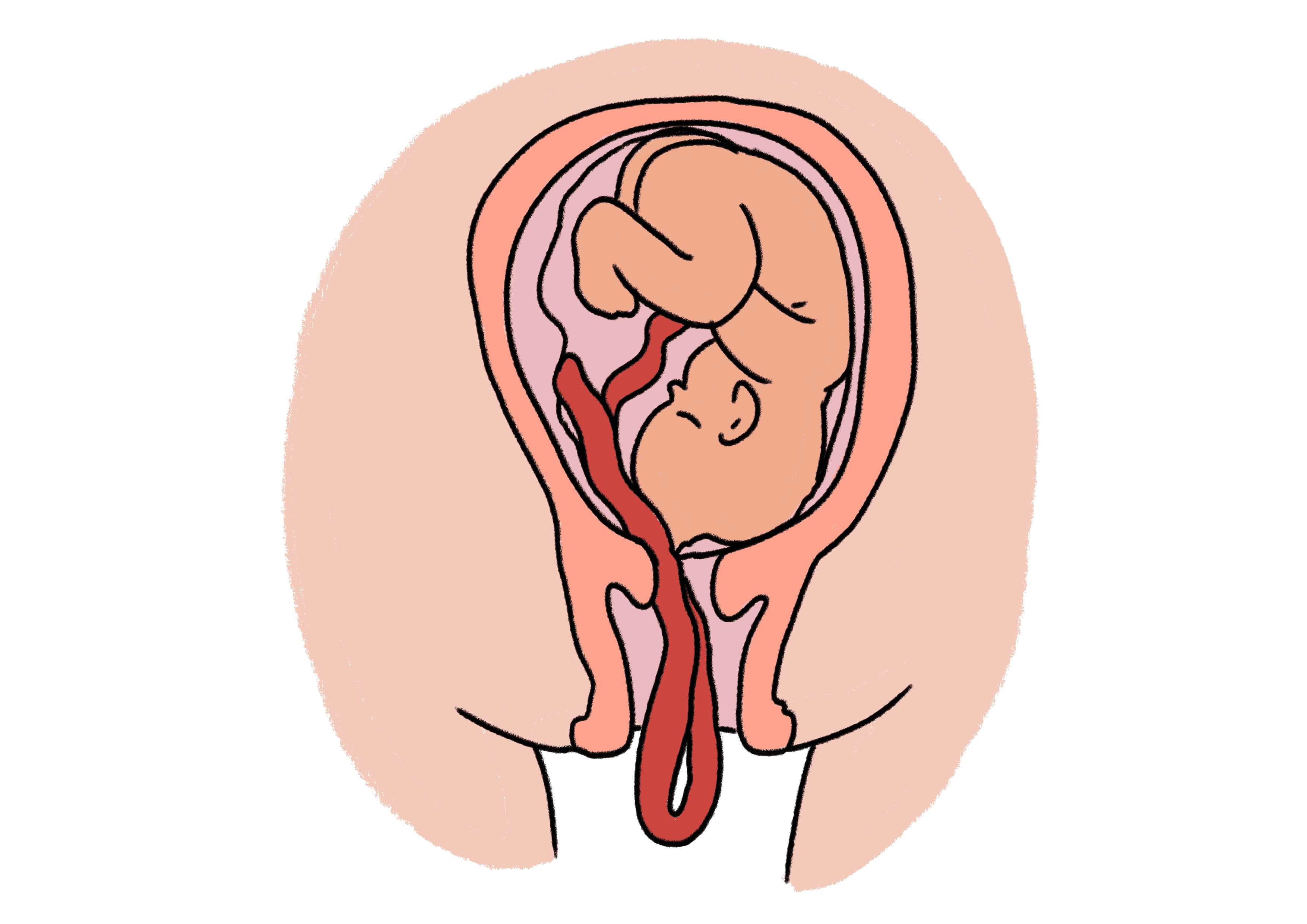
A cord prolapse is when the umbilical cord descends through the cervix (neck of the womb) alongside or in front of the leading part of the baby, either the head or buttocks after your waters have broken. This is an emergency because the cord can be compressed (blocked) and result in a lack of oxygen delivery to the baby.
There is a small chance (uncommon) of a cord prolapse occurring if your baby’s head is not engaged when we break your waters (artificial rupture of membranes), there is also a higher chance of cord prolapse if a balloon catheter is used to induce your labour and it is inflated too much - there are now safety features to prevent this happening. Other circumstances that have a higher chance of cord prolapse include, larger than average amount of amniotic fluid (polyhydramnios), if your baby is estimated to be less than 2.5kg (small for gestational age), and if you have had vaginal deliveries before.
Caesarean birth

You have a 25-30% chance of an unplanned or emergency c-section during your induction.
Reasons for this include:
Maternal choice.
You do not go into active labour during your induction.
If your baby is showing signs of distress e.g. pathological CTG.
If you become unwell during your labour e.g. suspected infection, high blood pressure/pre-eclampsia.
Cord prolapse.
Uterine rupture (if there is a scar on your womb).
Your likelihood of caesarean birth increases as your pregnancy continues beyond 41+0 weeks.
Shoulder Dystocia
Shoulder dystocia can occur during any vaginal delivery when you baby’s head delivers and there is a delay of their body birthing, requiring special manoeuvres to deliver your baby. This occurs in less than 1% of deliveries and is considered uncommon. Shoulder dystocia usually occurs unexpectedly, but it is more likely if:
Your body mass index is more than 30kg/m2.
You’ve had a previous shoulder dystocia.
You have diabetes mellitus or gestational diabetes.
Your baby is more than 4.5kg (large for gestational age).
You have an induction of labour.
You are given oxytocin to speed up your labour.
Your labour is longer than usual.
You have an instrumental birth.
Although induction is listed above, being induced earlier than 41 weeks may reduce your chance of shoulder dystocia if you have a large for dates baby, diabetes or gestational diabetes.
Placenta praevia, low-lying placenta or placental abruption

Your midwife/doctor is required to check that there is no evidence of a low-lying placenta on your previous ultrasound scans before induction of labour commences.
Signs of placenta praevia or abruption include vaginal bleeding with or without abdominal pains, or fetal distress. If there is a clinical suspicion of low-lying placenta or abruption, urgent medical review will be sought, and you may be advised to have an emergency caesarean section.
Uterine Rupture

You have a risk of uterine rupture if you have a scar on your womb from a previous caesarean section(s) or surgery on your uterus e.g. fibroid removal (myomectomy).
Your chance of uterine rupture is more likely if you are induced (4 in 1000 rather than 2 in 1000).
If this is suspected during your induction an emergency caesarean section will be advised. It is rare that there are serious consequences for you and your baby.
Red flags to alert midwifery/medical staff to during the induction
Please inform your midwife:
If you are in pain and this is distressing for you: there are plenty of options of pain relief available to you during your induction.
If you experience vaginal bleeding (antepartum haemorrhage) during your induction, your team will need to assess you, monitor you more closely or seek a review from an obstetric doctor. If the bleeding is considered significant, does not settle, and/or there are signs that your baby is in distress an emergency caesarean section will be advised.
If you have reduced fetal movements during your induction. Your midwife may need to monitor you more closely or seek a review from an obstetric doctor.
Labour can be stressful, get support if you feel anxious, have any queries or concerns.
References:
National Institute for Health and Care Excellence: Guidelines. Inducing labour. London: National Institute for Health and Care Excellence (NICE)
Middleton P, Shepherd E, Morris J, Crowther CA, Gomersall JC. Induction of labour at or beyond 37 weeks' gestation. Cochrane Database Syst Rev. 2020;7(7):Cd004945.
Harkness M, Yuill C, Cheyne H, McCourt C, Black M, Pasupathy D, et al. Experience of induction of labour: a cross-sectional postnatal survey of women at UK maternity units. BMJ Open. 2023;13(5):e071703.
RCOG. Birth After Previous Caesarean Birth 2015 [Available from: https://www.rcog.org.uk/media/kpkjwd5h/gtg_45.pdf.
Caesarean birth. London: National Institute for Health and Care Excellence (NICE); 2024 Jan 30. PMID: 33877751. Available from: https://www.nice.org.uk/guidance/ng192/chapter/Recommendations.
National Institute for Health and Care Excellence: Guidelines. Diabetes in pregnancy: management from preconception to the postnatal period. London: National Institute for Health and Care Excellence (NICE)
Li J, Shao X, Song S, Liang Q, Liu Y, Qi X. Immediate versus delayed induction of labour in hypertensive disorders of pregnancy: a systematic review and meta-analysis. BMC Pregnancy and Childbirth. 2020;20(1):735.
Morris RK, Johnstone E, Lees C, Morton V, Smith G, Obstetricians tRCo, et al. Investigation and Care of a Small-for-Gestational-Age Fetus and a Growth Restricted Fetus (Green-top Guideline No. 31). BJOG: An International Journal of Obstetrics & Gynaecology. 2024;131(9):e31-e80.
WHO Guidelines Approved by the Guidelines Review Committee. WHO recommendations on induction of labour, at or beyond term. Geneva: World Health Organization
Denison F, Aedla N, Keag O, Hor K, Reynolds R, Milne A, et al. Care of Women with Obesity in Pregnancy. BJOG: An International Journal of Obstetrics & Gynaecology. 2019;126(3):e62-e106.
RCOG. Umbilical Cord Prolapse 2014 [updated 2024. Available from: https://www.rcog.org.uk/media/3wykswng/gtg-50-umbilicalcordprolapse-2014.pdf.
RCOG. Shoulder Dystocia 2012 [Third:[Available from: https://www.rcog.org.uk/media/ewgpnmio/gtg_42.pdf.